Jump to:
After decades of raising awareness of sexual assault and focusing on improving the response to it, the elimination of sexual violence is being actively embraced as a goal by many sectors of society. Here in West Virginia, WVFRIS, rape crisis centers and other community organizations and professionals are using a variety of strategies to promote the change needed to end sexual violence. Facilitating the long-term shifts in community attitudes, norms and behaviors necessary to eradicate this problem is complex work, made all the more challenging because we are still learning what combinations of strategies are most effective in different settings. This section provides an overview of prevention principles that form the foundation of sexual violence prevention efforts.
Public Health Approach
Public health is described as “the science of protecting and improving the health of communities through education, promotion of healthy lifestyles and research for disease and injury prevention” (Association of Schools of Public Health). Two key aspects of a public health approach include:
- Public health focuses on the whole population’s health rather than single individuals.
- Public health is designed to counter threats to the public’s health and safety (PREVENT, 2005b; Turnock, 1997), such as sexual violence.
Public Health Process
Public health is focused on science, root causes and figuring out solutions to health problems based on evidence (WCSAP, 2012). Sexual violence is viewed as a preventable health problem.
A public health perspective asks foundational questions about sexual violence (Centers for Disease Control and Prevention—CDC’s The Public Health Approach to Violence Prevention):
- Where does the problem of sexual violence begin?
- How can we prevent sexual violence from occurring in the first place?
To answer these questions, public health relies on evidence. As the CDC explains, evidence is gathered to (1) define the extent of the problem, (2) identify factors that need to be addressed to reduce the problem’s occurrence and severity, and (3) test and develop prevention strategies. Then agencies that promote public health can (4) disseminate information about strategies deemed to be effective to those that implement prevention programs. They can also encourage monitoring and evaluation to assess impact and cost-effectiveness of each strategy.
Cultural Relevance
Public health also emphasizes a culturally appropriate response to health problems—recognizing that cultural practices and beliefs can influence the way data on the problem should be collected and how prevention programs are developed and disseminated (PREVENT, 2005b). Note that culture in this context does not refer only to ethnic or racial groups; it also to (Townsend, 2014):
- The ways members of a particular group or community live
- The types of activities that are valued within that community
- What makes members of the community feel welcomed and valued
- What makes a community organization appear credible
- How willing community members are to try new approaches
Continuum
From a public health perspective, there are three levels on the prevention continuum that focus on WHEN an intervention has an effect on sexual violence (PREVENT, 2005a):
- Primary prevention includes approaches that take place BEFORE sexual violence has occurred, to prevent initial perpetration or victimization. An example of an activity to prevent sexual violence is one that teaches students about healthy relationships and sexuality (adapted from Valle et al., 2007).
- Secondary prevention includes immediate responses AFTER sexual violence has occurred, to deal with the short-term consequences. Examples might include crisis intervention, advocacy and medical care for a victim, SANE (sexual assault nurse examiner) programs to improve the collection of forensic evidence, and the development of SARTs (sexual assault response teams) to create a collaborative multidisciplinary response.
- Tertiary prevention includes long-term responses AFTER sexual violence, to deal with the lasting consequences, with the goal of lessening the long-term effects and reducing the chances of reoccurrence. Tertiary prevention is designed to address problems through policies, programs and services for people who have already experienced a problem (e.g., those who have been victimized by sexual violence and those who have perpetrated sexual violence). Examples are counseling services and self-defense classes for survivors and sex offender treatment programs.
Categories
Sexual violence prevention interventions can also be divided into the three categories, based on WHO is at risk for victimization or perpetration and to whom primary prevention efforts should be directed (CDC, 2004; PREVENT, 2005a):
- Universal interventions are directed at groups or the general population regardless of individual risk for sexual violence perpetration or victimization. Examples of universal interventions might include public awareness campaigns about sexual violence and reducing sexual violence in media. In universal interventions, everyone is protected, and everyone shares the burden of the intervention.
- Selected interventions target those who are thought to have a heightened risk for sexual violence perpetration or victimization. Selected interventions might include activities targeting adolescents who use drugs/alcohol or sexuality education for persons with intellectual disabilities
- Indicated interventions are directed at those who have already perpetrated sexual violence or have been victimized. Examples of indicated interventions might be counseling services and crisis intervention for victims, incarceration of perpetrators or school-wide discussions following school-based sexual assault.
Primary prevention targets universal and selected approaches, since their focus is to stop violence before it occurs (PREVENT, 2005a). The differentiation between universal and selected approaches speaks to the dilemma of viewing sexual violence as a problem facing all members of society while acknowledging that specific populations are more at risk for being victims or perpetrators.
Primary Prevention
Impact of Primary Prevention
“There is an often-quoted parable that tells of a man and woman fishing downstream. Suddenly a person comes down the river struggling for life. The fisherfolk pull her out. Then another comes and again must be rescued. This happens all afternoon and the fisherfolk are getting very tired from constantly pulling people from the river.
When they go upstream, they find that people are drawn to the edge to look at the river, but there is no safe way to do this. Many of them fall. The fisherfolk go to the community leaders and report the number of people who have fallen into the river. They also report that this is due to the lack of a protective barrier on the cliff. Community leaders build a wall behind which people may safely view the water. Some still fall, but there are many fewer victims to rescue.”
CDC, 2004; PREVENT, 2005a.
From the fisherfolk’s tale, we can identify several key components of prevention (CDC, Principles of Prevention Guide): First, the fisherfolk identified the problem—people were falling into the river. Next, the fisherfolk did a thorough investigation and found a problem with the trail that put people at risk for falling into the river. The fisherfolk’s solution involved enlisting the help of neighbors to build a fence that would keep people out of the river. After putting the fence in place and seeing that no one else had fallen into the river, the fisherfolk were able to determine that the solution was successful and future problems were prevented. The fisherfolk employed a primary prevention approach to stop the problem from happening in the first place, instead of expending all resources and energy on rescuing people who have fallen into the river (PREVENT, 2005a).
Reshaping Environment and Norms
(Adapted from Lyle, Cohen & Brown, 2009)
A primary prevention approach to sexual violence promotes safe, healthy environments and behaviors, reducing the likelihood of violence occurring in the first place. This approach is sometimes confused with early intervention services for victims and perpetrators that are implemented after violence occurs that seldom alter social norms that support or tolerate sexual violence.
If sexual violence is typical, expected and reinforced by the media, family, community, peers or school, it is more likely to occur. If the environment and norms discourage safe behavior and don’t support healthy relationships, then prevention efforts will not produce safe behavior. However, primary prevention moves “upstream” to change the environmental factors that shape community norms and behaviors. The primary prevention of sexual violence is a systemic process capable of reshaping norms.
Given the challenge of changing the environment and norms, it is essential to view sexual violence prevention not as a one-time, one skill-building effort. Rather, it is an ongoing, multi-faceted process.
Risk and Protective Factors
A primary prevention approach typically employs a variety of strategies to counteract the root causes of a specific problem (PREVENT, 2005a), addressing related risk factors and promoting protective factors:
- A risk factor is a behavior or condition that increases vulnerability to a specific condition (see below).
- A protective factor is a behavior, social influence or policy that reduces vulnerability to a specific condition or other behaviors.
In sexual violence primary prevention efforts, stopping initial perpetration of sexual violence is the focus. The presence or absence of certain risk factors can increase or decrease the likelihood that someone may become a perpetrator of sexual violence. Knowing the factors that lead to perpetration can raise awareness about the issue and aid in planning prevention strategies to help stop sexual violence before it starts. Similarly, protective factors for sexual violence may decrease the likelihood of perpetration or victimization. (Paragraph from Veto Violence).
Social Ecological Model
The public health approach to sexual violence prevention is driven by a social ecological model that outlines how the health status of a person is influenced not just by that person’s attitudes and practices, but also by personal relationships and community and societal factors (PREVENT, 2005c).
A core tenet of this model is that human behavior does not happen in a vacuum (Guy, 2007). People perpetrate sexual violence for a wide variety of reasons and as a result of many different influences on their lives—the social ecological model provides a framework for understanding those different reasons and influences. (Paragraph from WCSAP, 2012)
Levels of Risk
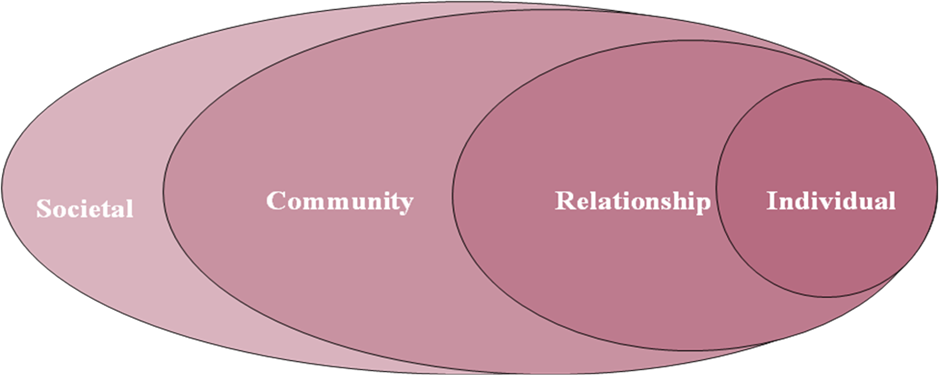
The World Health Organization (WHO), in World Report on Violence and Health (Krug et al., 2002), used a variation of this model to discuss violence prevention. (See below for an illustration of this model from that report.) The CDC then used this model to delineate specific risk factors for perpetration of sexual violence (CDC, 2004):
- Individual level—biological and personal history factors that increase the likelihood of becoming a perpetrator of violence. Risk factors include but are not limited to alcohol and/or drug use, attitudes and beliefs that support sexual violence, impulsive and other antisocial tendencies, preference for impersonal sex, hostility towards women, and childhood history of sexual abuse or witnessing family violence (Krug et al., 2002). An individual may also be influenced by demographic characteristics such as age, income and education (PREVENT, 2005c).
- Relationship level—factors that increase risk because of relationships with peers, intimate partners and family members. These relationships can shape an individual’s behavior and range of experience (Krug et al., 2002).
- Community level—settings in which social interactions occur (e.g., schools, churches, neighborhoods and workplaces) and characteristics of these settings that are associated with becoming perpetrators of violence. For example, the lack of workplace policies on sexual harassment can send a message that this type of violence is tolerated.
- Societal level—broad societal factors that create a climate in which violence is encouraged or inhibited. Risk factors include but are not limited to gender inequality, religious or cultural belief systems, societal norms and economic or social policies that create or sustain gaps and tensions between groups of people.
Influencing Culture and Behavior
Addressing sexual violence prevention requires acknowledging that factors influencing perpetration fall along the entire social ecological model (WCSAP, 2012). In fact, risk factors work together to influence culture and behaviors related to sexual violence perpetration (CDC, 2004). The model highlights the pivotal role that societal factors play in influencing behaviors and interactions between people and entities (PREVENT, 2005c).
Multiple Strategies
Ideally, to work to prevent sexual violence, multiple prevention strategies and activities simultaneously occur at different levels of the social ecological model. The key is to understand that different levels of the model can reinforce different aspects of a prevention message and to utilize multiple levels in prevention efforts.
Spectrum of Prevention
The “spectrum of prevention” (based on Cohen & Swift, 1999) offers a framework to develop multi-level prevention strategies that are aligned with the social ecological model. In this framework, six levels of the spectrum define distinct strategies to prevent sexual violence—by reducing risk factors and/or increasing protective factors. Each level can be addressed using multiple approaches and activities. Here are the levels and goals of each (National Sexual Violence Resource Center or NSVRC, 2011):
- Strengthening individual knowledge and skills
- Promoting community education
- Educating service providers/professionals
- Fostering coalitions and networks
- Changing organizational practices
- Influencing policy and legislation
Note that the CDC developed STOP SV: A Technical Package to Prevent Sexual Violence (2016) to help communities take advantage of the best available evidence to prevent sexual violence. The included strategies (below) are intended to impact individual behaviors as well as the relationship, family, school, community and societal factors that influence risk and protective factors for violence.
- Promote social norms that protect against violence
- Teach skills to prevent sexual violence
- Provide opportunities to empower and support girls and women
- Create protective environments
Programming
A range of types of sexual violence prevention program approaches and activities can be tailored to target populations and settings. For example:
- Curriculum-Based Instruction
- Educational sessions
- Bystander intervention approaches
- Programs that mobilize boys/men to take an active role in stopping sexual violence
- Professional trainings
- Social norms campaigns
- Mobilization of the community around sexual violence prevention
- Community mobilization
- Collaboration with community groups
- Promotion of systems change
What Makes a Prevention Program Effective?
Nine principles of effective prevention programs were identified in What Works in Prevention: Principles of Effective Prevention Programs (Nation et al 2003):
- Comprehensive methods (using multiple strategies in multiple settings to address different aspects of a person’s life)
- Varied teaching methods (to reach all types of learners, including those who need interactive methods to practice skill development)
- An adequate number of activities (enough for someone to understand the information and change their behavior/beliefs)
- A theory base (either scientifically proven/evaluated or supported by a logic model)
- Promoting positive relationships (e.g., between children and adults)
- Developmentally appropriate and pertinent material
- Cultural relevance
- An evaluation component that examines outcomes, not just counting the number of people who attend
- Presenters/facilitators who are competent, trained, sensitive to the issue and have the support they need to be effective
Thoughtful, well-planned prevention programs that are intentional in both addressing factors to maximize their effectiveness as well as targeting multiple levels on the social ecological models will enable us to reach our ultimate goal: no more victims of sexual violence.
Primary Prevention, Awareness and Outreach or Risk Reduction
How do primary prevention activities differ from sexual violence awareness and outreach activities and risk reduction activities? Curtis and Love (2011) noted differences in goals across these activities.
- Primary prevention goals: Eliminate and reduce factors that perpetuate sexual violence to keep it from happening in the first place; create healthy norms and healthy communities.
- Awareness and outreach goals: Tell the community that sexual violence exists and reach out to victims so that they will seek services.
- Risk reduction goals: Thwart an attack that is in process, avoid imminent attacks or avoid dangerous people/ situations. (Remember that the priority in prevention is working to prevent initial perpetration rather than how victim activities might reduce victim risk. If risk reduction activities are employed, programmers must understand potential problems and plan to counter them. See below.)
Risk Reduction Tips
These tips should not be offered in isolation from other prevention strategies, as alone they send the inaccurate message that it is up to individuals to avoid victimization. If risk reduction strategies are offered, they should be just one component of a comprehensive sexual violence prevention programming.
Sexual violence is never the victim’s fault; however, taking these precautions could potentially reduce your risk of being assaulted.
- Trust your instinct. If you don’t feel comfortable in a situation, leave.
- Stay in charge of your own life. If possible, don’t put yourself in situations where you have to rely on others financially or for housing or are made to feel you “owe” someone.
- Be cautious inviting someone into your home or going to someone else’s home.
- Do not mix sexual decisions with drugs and alcohol.
- When going out with someone new, go out with a group or meet in a public place.
- Be aware of drugs used to facilitate sexual assault. Don’t accept beverages from open containers and don’t leave your drink unattended.
- Do not be pressured by lines such as, “If you loved me.” If your partner loved you, they would respect your feelings.
- Avoid individuals who:
- Don’t respect you
- Ignore personal boundaries
- Make you feel guilty or accuse you of being “uptight” for resisting sexual advances
- Express sexist attitudes and jokes
- Are jealous or possessive
- Communicate. Think about what you want before you get into a sexual situation. Clearly and assertively communicate your feelings to your partner or date.
Resources
References
Association of Schools of Public Health. (n.d.). What is public health? Washington, DC.
Centers for Disease Control and Prevention (CDC). (2009). Sexual violence: Risk and protective factors. Atlanta, GA.
Centers for Disease Control and Prevention (CDC). (2004). Sexual violence prevention: Beginning the dialogue. Atlanta, GA: Author
Centers for Disease Control and Prevention (CDC). (n.d.). The public health approach to violence prevention. Atlanta, GA: Author.
Centers for Disease Control and Prevention (CDC). (n.d.). The social ecological method: A framework for violence prevention. Atlanta, GA: Author.
Cohen, L. & Swift, S. (1999). The spectrum of prevention: Developing a comprehensive approach to injury prevention. Injury Prevention, 5, 203-7.
Curtis, M. & Love, T. (2011). Tools for change: An introduction to the primary prevention of sexual assault. Austin, TX: Texas Association Against Sexual Assault.
Guy, L. (2007). The ecological model of health behavior: An overview for advocates. Washington Coalition of Sexual Assault Programs Partners in Social Change, 9(3), 4-6.
Krug, E., Dahlberg, L., Mercy, J., Zwi, A. & Lozano, R. (Eds.) (2002), World report on violence and health. Geneva, Switzerland: World Health Organization, 3-21.
Lyles, A., Cohen, L., & Brown, M. (2009). Transforming communities to prevent child sexual abuse and exploitation: A primary prevention approach. Oakland, CA: Prevention Institute.
Nation, M., et al. (2003). What works in prevention: Principles of effective prevention programs. American Psychologist, 58, 449-456.
National Sexual Violence Resource Center (NSVRC). (2011). Fact sheet: Sexual violence and the spectrum of prevention. Enola, PA: Author.
PREVENT. (2009). Prevent facilitator toolkit. Raleigh, NC: University of North Carolina Injury Prevention Research Center.
PREVENT. (2005a). Orientation to violence prevention. Moving upstream: The story of prevention. Raleigh, NC: University of North Carolina Injury Prevention Research Center.
PREVENT. (2005b). Orientation to violence prevention. The public health approach to violence prevention. Raleigh, NC: University of North Carolina Injury Prevention Research Center.
PREVENT. (2005c). Orientation to violence prevention. The social ecological model: A pathway to prevention. Raleigh, NC: University of North Carolina Injury Prevention Research Center.
Townsend, S. (2014). Choosing prevention strategies (Vol. 1). Primary prevention and evaluation resource kit. Enola, PA: Pennsylvania Coalition Against Rape.
Turnock, B. (1997). Public health: What it is and how it works. Baltimore, MD: Aspen.
Valle, L., Hunat, D., Costa, M., Shively, M., Townsend, M., Kuck, S., Rhoads, W. & Baer, K. (2007). Sexual and intimate partner violence prevention programs evaluation guidebook. Atlanta, GA: Centers for Disease Control and Prevention .
Veto Violence. (n.d.). Sexual violence [Webpage]. Centers for Disease Control and Prevention.
Veto Violence. (n.d.). The levels of prevention [Webpage]. Centers for Disease Control and Prevention.
Virginia Sexual and Domestic Violence Action Alliance. (2009). Virginia’s guidelines for the primary prevention of sexual violence & intimate partner violence. Richmond, VA: Author.
Washington Coalition of Sexual Assault Programs (WCSAP). (2012). Prevention orientation [Online course]. Olympia, WA: Author.
Washington Coalition of Sexual Assault Programs (WCSAP). (n.d.) The social ecological model. Olympia, WA: Author.
World Health Organization. (2002). Sexual violence facts. Data from Krug et al.